Volume 1, Issue 2
Article Type: Research Article
The elderly waiting for dental treatment and the risk of geriatric syndromes
Erik Dreyer*; Braulio Santibáñez; Natalia Salazar; Angélica Michea; Pilar Barahona; Paula Van Treek; Andrés Celis
Dental Faculty, University of Chile, Chile.
*Corresponding author: Erik Dreyer
Dental Faculty, University of Chile, Chile.
Tel:Email ID: edreyer@odontologia.uchile.c
Received: Jun 24, 2025
Accepted: Jul 23, 2025
Published Online: Jul 30, 2025
Journal: Annals of Gerontology and Geriatrics
Copyright: Dreyer E et al. © All rights are reserved
Citation: Dreyer E, Santibanez B, Salazar N, Michea A, Barahona P, et al. The elderly waiting for dental treatment and the risk of geriatric syndromes. Ann Gerontol Geriatr Res. 2025; 1(2): 1013.
Abstract
Purpose: To determine the risks of geriatric syndromes, including falls, depression, dependence, polypharmacy, sarcopenia, and malnutrition, in older individuals on the waiting list. Methods: The sample consisted of 124 elderly Chilean participants aged 70 and above. The Timed Up-andGo test was utilized to evaluate the risk of falls. Masticatory function was assessed based on the number of remaining teeth and the Eichner Index. Regression models were employed to analyze the relationships between participants’ characteristics and the risk of geriatric syndromes. Results: Significant differences in the distribution of risks for the syndromes were assessed, revealing that a significantly higher proportion of individuals were at no risk, with falls being the exception. Older age was associated with an increased risk of falls, dependence, sarcopenia, and malnutrition. The risk of sarcopenia was significantly linked to a lower average number of remaining teeth. Conclusion: Significant disparities were noted in the risk distribution of all syndromes, with the absence of risk being the most common, except for falls. The findings underscore the importance of incorporating geriatric syndromes into oral health strategies.
Keywords: Geriatric syndromes; Population aging; Oral functionality.
Introduction
The extension of human longevity and the decline in fertility rates have inevitably led to a demographic transition, in which older individuals have gained increasing significance within the population’s age structure [1]. Over the past 50 years, life expectancy at birth has increased dramatically, rising from 57.3 years at the beginning of the 1960s to 79.5 years today [2].
Chile has also experienced this trend, especially over the past decade, with this age group making up 18.1% of the country’s total population by 2022. According to projections, its share is expected to double by 2050, reaching about one-third of the population (32.1%) [3]. Aging is closely linked to high multimorbidity [2], a pattern that increases among the elderly, particularly those from lower socioeconomic backgrounds.
The decline in physical and mental health that accompanies aging, along with the increase in chronic diseases, can lead to a gradual loss of independence and function unless specific interventions are implemented to prevent it. The term “geriatric syndromes” describes clinical conditions in older adults that do not fit into traditional disease categories. These syndromes, which have multifactorial causes, greatly affect quality of life and disability in older adults. The most important geriatric syndromes include falls, depression, frailty, dependency, polypharmacy, sarcopenia, delirium, neurocognitive disorder, and malnutrition.
Data from the ‘GLOSA 06’ report, issued by the Chilean subsecretariat of Healthcare Networks, shows that the number of patients awaiting oral rehabilitation increased from 126,083 in 2018 to 132,110 in 2019. However, the subsequent years saw a gradual decrease, with 121,236 cases in 2020, 113,137 in 2021, and 110,894 in 2022 [6]. The reduction in cases on the waiting list since 2020 aligns with the COVID-19 pandemic years, during which mortality from this disease significantly affected the older population.
However, at the national level, research on the prevalence of geriatric syndromes among edentulous individuals remains limited. This gap in evidence is particularly concerning given that oral rehabilitation has the longest waiting list among all dental specialties in the country. Therefore, this study aimed to evaluate the risk of geriatric syndromes, including falls, depression, dependency, polypharmacy, sarcopenia, and malnutrition, in older adults awaiting dental prosthesis rehabilitation within the Chilean public health system.
Materials
This study was an observational, quantitative, cross-sectional, and analytical research project. The final sample corresponds to the FONIS SA20I0052 Project, which included 124 individuals aged 70 and older who utilized the dental service at Hospital del Salvador. These individuals were on the waiting list for dental care, referred from Primary Health Care, and were about to begin prosthetic rehabilitation treatment. Ethics approval for this study was granted by the Ethics Committee of the Eastern Metropolitan Health Service, which supervises the research (approval number 722023).
Data were collected at the Dental Service of Hospital del Salvador from 2021 to 2023. The inclusion criteria encompassed individuals aged 70 years and older, patients referred from Primary Health Care who were on the waiting list for dental treatment in the prosthetics specialty of the dental service at Hospital Del Salvador, and patients classified under the Eichner [7] classification groups B3, B4, C1, C2, and C3. The exclusion criteria included patients with moderate to severe cognitive impairment, as measured by the Pfeiffer scale, those unable to perform facial movements due to degenerative diseases, and individuals with soft tissue pathologies such as fibromas, fissured epulis, and hyperplasias.
The risk of falls was assessed using the Timed Up and Go test, which involved using a stopwatch to measure how long it took for the patient to rise from a chair, walk to a marker located three meters away, turn around, and return to the chair while using their usual assistive device, such as a cane or walker. Based on the total time, the patient was classified into three risk levels: normal if it took ≤10 seconds, low risk of falls if it took 11 to 20 seconds, and high risk of falls if it took >20 seconds [8].
The risk of depression was assessed using the Geriatric Depression Scale-5 (GDS-5), which is a valid and reliable measure for evaluating depression risk in older adults. Participants were asked to answer five questions regarding how they felt over the past week [9].
Are you generally satisfied with your life? Do you frequently feel bored?
Do you often feel worthless?
Do you prefer staying home instead of going out and trying new things?
Do you often feel helpless or worthless?
Participants were asked to respond with “yes” or “no” to each question. A positive response to depression included “no” for the first question and “yes” for the subsequent questions. Two or more positive responses to depression were considered indicators of depressive symptoms (≥2 points) [10].
The risk of dependence was measured using the Lawton and Brody scale [11], which evaluates functional capacity through a series of questions that assess an individual’s independence in performing various instrumental activities of daily living. These activities include, but are not limited to, using the telephone, shopping, preparing meals, doing housework, doing laundry, using transportation, managing medications, and handling financial responsibilities. Each activity was assessed on a scale ranging from complete independence to complete dependence, providing a quantitative measure of an individual’s functional autonomy. Scores typically range from 1 to 8, with 8 points indicating complete independence in all assessed activities. 7 points: Partial dependence on one or more activities. 6 points or fewer: Significant reliance on several activities, indicating various levels of need for assistance.
To assess the presence of polypharmacy, the total number of medications taken by each participant was recorded. Polypharmacy was defined as the use of more than five different medications simultaneously, following the parameters set by the World Health Organization [12].
Handgrip strength, which serves as a measure of sarcopenia risk, was assessed with the prostheses in occlusion using a hydraulic hand dynamometer (Jamar MR) for 2 to 3 seconds. Three measurements were taken, and the highest value was recorded. According to the European Working Group on Sarcopenia in Older People, the risk of sarcopenia was considered when grip strength levels were ≤27 kg for men and ≤16 kg for women [13,14]. Calf circumference served as a nutritional indicator and was measured at the highest point of the calf or midway between the knee and the base of the heel. The sole criterion for categorizing this indicator was that a measurement of less than 31 cm was considered indicative of malnutrition [15].
The data collected during clinical procedures were stored in an Excel spreadsheet (Microsoft Corporation, CA, USA) for further analysis. The chi-square test was used to assess the proportion of patients in the sample at risk for geriatric syndromes compared to those not at risk, based on the selected indicators, to determine whether there was a higher proportion of participants classified as “at risk” for developing geriatric syndromes. Finally, all analyses were performed using SAS 9.4 software (SAS Institute Inc., Cary, NC, USA), with a statistical significance level of 95% (p<0.05).
Results
The sample included 124 participants, comprising 73 females (59%) and 51 males (41%) (Table 1). A chi-square test was conducted to evaluate the gender distribution within the sample, revealing a significant difference in the proportion of female to male participants (p=0.0482). The average age of the participants was 81.2±5.9 years, ranging from 71 to 97 years. When the data were analyzed by sex, the average age for women was 80±3.9 years, with a range of 71 to 97 years. In contrast, the average age for men was 82±6.1 years, within a range of 71 to 96 years. No significant differences were found in the ages regarding sex (p=0.0734).
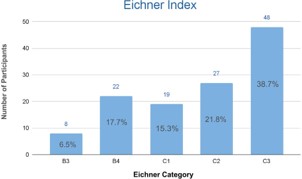
The masticatory function was assessed using the Eichner index. Among participants, 38.7% were classified as C3, 21.8% as C2, 17.7% as B4, 15.3% as C1, and 6% as B3, with B3 being the least represented. Additionally, the Chi-square test indicated that category C3 had the highest representation in the sample (p<0.0001) (Figure 1).
In terms of fall risk, 90% of older adults in the sample were classified as being at either slight or high risk, with 14% falling into the high-risk category. The distribution differed significantly from those classified as not at risk (p<0.0001) (Table 2).
Regarding the risk of depression, a significant 73% were not at risk, and the chi-square test showed notable differences in distribution compared to those at risk (p<0.0001) (Table 2). When assessing the risk of dependency, 58% of the sample was classified as independent, with no significant differences identified between those categorized as independent and those with some degree of dependency (p=0.0725). However, when distinguishing between different degrees of dependency and comparing them to the percentage of independent individuals, significant differences in risk distribution were observed (p<0.0001) (Table 2).
Similarly, when assessing polypharmacy, 59% did not exhibit polypharmacy (p=0.0483) (Table 2).
Concerning the risk of sarcopenia and malnutrition, the percentage of participants not at risk for these conditions was 61% and 96%, respectively. Additionally, the application of the chi-square test revealed significant differences in the distribution of risk for both geriatric syndromes (p=0.0119 and p<0.0001, respectively).
Table 1: Demographic characteristics by sex and age.
| Sex | AGE (years) | |||||
|---|---|---|---|---|---|---|
| Frequency | Percentage | P-value | Mean | Median | P-Value | |
| Males | 73 | 58.87% | 0.0482 | 82.4 (±6.1) | 83 | 0.0734 |
| Females | 51 | 41.13% | 80.4 (±5.8) | 80 | ||
| Total sample | 124 | 100% | 81.2 (±5.9) | 81 | ||
Table 2: Risk assessment of geriatric syndromes according to their respective indicators.
| Risk of geriatric syndromes | |||
|---|---|---|---|
| Frecuency | Percentage | P-Value | |
| Risk of falls by timed up and go | |||
| Normal | 13 | 10.48% | |
| Mild | 94 | 75.81% | |
| High | 17 | 13.71% | < 0.0001 |
| Some degree of risk (not categorized) | 111 | 89.52% | < 0.0001 |
| Depression risk by GDS-5 | |||
| No | 90 | 72.58% | < 0.0001 |
| Yes | 34 | 27.42% | |
| Risk of dependency by Lawton & Brody | |||
| Autonomous | 72 | 58.06% | < 0.0001 |
| Mild dependency | 33 | 26.61% | |
| Moderate dependency | 12 | 9.68% | |
| Severe dependency | 5 | 4.03% | |
| Total dependency | 2 | 1.61% | |
| Some degree of dependency | 52 | 41.94% | 0.0725 |
| Polypharmacy by to the number of drugs administered | |||
| No | 73 | 58.87% | |
| Yes | 51 | 41.13% | 0.0482 |
| Sarcopenia risk by handgrip strength | |||
| No | 76 | 61.29% | |
| Yes | 48 | 38.71% | 0.0119 |
| Risk of malnutrition by calf circumference | |||
| No | 119 | 95.97% | |
| Yes | 5 | 4.03% | < 0.0001 |
Discussion
The present study aimed to evaluate the risk of geriatric syndromes in older adults on the waiting list for dental prosthesis rehabilitation within the Chilean public health system. To this end, relevant medical history previously recorded at baseline was collected to estimate the risk of these syndromes before beginning rehabilitation treatment. These included risks of falls, depression, dependency, polypharmacy, sarcopenia, and malnutrition. The results indicated significant differences in the risk distribution of all analyzed geriatric syndromes.
The assessment of masticatory function revealed that the entire sample had non-functional dentition, consistent with their status on the waiting list for prosthetic rehabilitation. Additionally, a majority (39%) of the participants were completely edentulous, classified as C3 according to Eichner, which aligns with national data on edentulism from the 2016-2017 National Health Survey, which reported a total edentulism rate of 41.2% in the population aged 75 years or older [16].
Regarding the risk of falls, a higher proportion of patients were identified as at risk. Specifically, 90% of the sample was at risk of falling. This percentage considerably exceeds the prevalence of 35.3% among older adults in Chile, as reported in 2001 by the Health, Well-being, and Aging Survey (SABE) [17]. Although the risk of falls is known to increase with age, the high risk observed in the sample is concerning and should be considered by healthcare providers, as falls in older adults can be very harmful, indicating possible undetected pathologies or frailty, and also serve as a predictor of mortality. On the other hand, 73% of the sample did not present a risk of depression. However, the 27% at risk exceeds the 21% prevalence reported in the Survey on the Quality of Life of Older Adults of Chile [8]. This aligns with a national study based on data from the last National Health Survey in Chile, 2016-2017, which concluded that frequent discomfort related to prostheses or teeth while eating was linked to a higher frequency of suspected or diagnosed depression in the previous 12 months [19]. Our results also numerically exceed the frequency of depression found in a Japanese study, which concluded that the deterioration of oral function and orofacial appearance mediated the relationship between tooth loss and depression in older adults [20].
Conclusion
Significant differences were noted in the risk distribution of all analyzed geriatric syndromes, with the absence of risk being the most common, except for the risk of falls. In the geriatric context, particularly within the public health system, it is crucial to recognize the substantial disease burden affecting this age group. Embracing an interdisciplinary approach to timely dental care aids in identifying risk factors for various diseases. This optimizes prevention and treatment strategies, enhancing both oral health and the overall well-being of patients. Such an approach leads to more comprehensive and higher-quality care for the older population.
Declarations
Authorship and ethical considerations: All co-authors approved the final version of the manuscript entitled “The Elderly Waiting for Dental Treatment and the Risk of Geriatric Syndromes” before submission and declared no conflict of interest. The Eastern Metropolitan Health Service Ethics Committee approved the clinical trial (approval number: 722023), which was subsequently registered in the U.S. National Library of Medicine clinical trials database (ClinicalTrials.gov identifier: NCT05818436).
References
- Rojas FH, Canache LR, León JR. Aging in Chile: Evolution, characteristics of older adults, and demographic challenges for the population [Internet]. Santiago: Department of Demographic and Social Statistics, National Institute of Statistics. 2022.
- Ministerio de Salud, Subsecretaría de Salud Pública. National comprehensive health plan for older people and its 2020–2030 action plan. Santiago: Gobierno de Chile. 2021.
- Albala C. The aging of the Chilean population and the challenges for the health and well-being of older people. Rev Méd Clín Las Condes. 2020; 31: 7–12.
- Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, et al. Aging with multimorbidity: A systematic review of the literature. Ageing Res Rev. 2011; 10: 430–9.
- Inouye SK, Studenski S, Tinetti ME, Kuchel GA. Geriatric Syndromes: Clinical, Research, and Policy Implications of a Core Geriatric Concept. J Am Geriatr Soc. 2007; 55: 780–91.
- Ministerio de Salud, Gobierno de Chile. Technical guidance for comprehensive care for fragile elderly people in acute geriatric units (AGU). Santiago: MINSAL. 2018.
- Ministerio de Salud de Chile, Subsecretaría de Redes Asistenciales. Glosa O6: Lista de espera No GES y Garantías de Oportunidad GES Retrasadas. 2018.
- Ministerio de Salud de Chile, Subsecretaría de Redes Asistenciales. Glosa O6: Lista de espera No GES y Garantías de Oportunidad GES Retrasadas. 2019.
- Ministerio de Salud de Chile, Subsecretaría de Redes Asistenciales. Glosa O6: Lista de espera No GES y Garantías de Oportunidad GES Retrasadas. 2020.
- Ministerio de Salud de Chile, Subsecretaría de Redes Asistenciales. Glosa O6: Lista de espera No GES y Garantías de Oportunidad GES Retrasadas. 2021.
- Ministerio de Salud de Chile, Subsecretaría de Redes Asistenciales. Glosa O6: Lista de espera No GES y Garantías de Oportunidad GES Retrasadas. 2022.
- Eichner K. Renewed examination of the group classification of partially edentulous arches by Eichner and application advices for studies on morbidity statistics. Stomatol DDR. 1990; 40: 321– 5.
- Podsiadlo D, Richardson S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991; 39: 142–8.
- Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: A preliminary report. J Psychiatr Res. 1982; 17: 37–49.
- Rinaldi P, Mecocci P, Benedetti C, Ercolani S, Bregnocchi M, Menculini G, et al. Validation of the Five-Item Geriatric Depression Scale in elderly subjects in three different settings. J Am Geriatr Soc. 2003; 51: 694–8.
- Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969; 9: 179–86.
- World Health Organization (WHO). Medication safety in polypharmacy: Technical report. Geneva: WHO. 2019.
- Dodds RM, Syddall HE, Cooper R, Benzeval M, Deary IJ, Dennison EM, et al. Grip strength across the life course: Normative data from twelve British studies. PLoS One. 2014; 9: e113637.
- Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing. 2019; 48: 16–31.
- Pinheiro AC, Scarpelli Dourado DAQ, Masferrer Riquelme DA. Manual de evaluación nutricional. Santiago: MINSAL. 2022.
- Ministerio de Salud de Chile, Departamento Salud Bucal. Comprehensive oral health clinical practice guide: Oral treatment and rehabilitation in adults and older adults with partial or total edentulism. Santiago: MINSAL. 2020.
- DIPRECE. Tratamiento y Rehabilitación Oral en Personas Adultas y Personas Mayores con Edentulismo Parcial o Total. Santiago: MINSAL. 2018.
- Subsecretaría de Previsión Social. Survey on the quality of life of older adults and the impact of the solidarity pillar. Santiago: Gobierno de Chile. 2018.
- Palomer T, Ramírez V, Ortuño D. Relationship between oral health and depression: Data from the National Health Survey 2016–2017. BMC Oral Health. 2024; 24: 188.
- Kusam T, Kiuchi S, Umehara N, Kondo K, Osaka K, Aida J. The deterioration of oral function and orofacial appearance mediated the relationship between tooth loss and depression among community-dwelling older adults: A JAGES cohort study using causal mediation analysis. J Affect Disord. 2021; 286: 174–9.