Volume 1, Issue 2
Article Type: Research Article
Outcome measures utilised in studies evaluating comprehensive geriatric assessment based perioperative medicine services: A scoping review
Garry Mallett1*; Olivia Flynn1; Judith SL Partridge1,2; Jugdeep K Dhesi1,2
1Perioperative Medicine for Older People Undergoing Surgery (POPS), Department of Ageing and Health, Guy’s and St Thomas’ NHS Foundation Trust, London, UK.
2School of Life Course and Population Sciences, Faculty of Life Sciences and Medicine, King’s College London, London, UK.
*Corresponding author: Garry Mallet
Perioperative Medicine for Older People Undergoing
Surgery (POPS), Department of Ageing and Health, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
Tel: +447922506259, Email ID: garry.mallett@nhs.net
Received: Jun 24, 2025
Accepted: Jul 30, 2025
Published Online: Aug 06, 2025
Journal: Annals of Gerontology and Geriatrics
Copyright: Mallett G et al. © All rights are reserved
Citation: Mallett G, Flynn O, Partridge JSL, Dhesi JK. Outcome measures utilised in studies evaluating comprehensive geriatric assessment based perioperative medicine services: A scoping review. Ann Gerontol Geriatr Res. 2025; 1(2): 1014.
Abstract
Background: Integrating Comprehensive Geriatric Assessment (CGA) into the surgical pathway for older adults has been variably achieved. Dissecting this variability, and assessing the effectiveness of CGA-based services, is challenging due to a lack of standardised outcome measures. We report a scoping review of studies evaluating perioperative CGA to describe previously utilised outcome measures.
Objective: To describe outcome measures used to examine the impact of CGA-based perioperative medicine services.
Methods: Using scoping review methodology, we systematically searched published studies examining CGA-based perioperative medicine services in three electronic databases (Embase/MEDLINE/Web of Science), supplemented with relevant reference lists. Verbatim outcome measures were extracted, standardised, and mapped into pre-defined domains adapted from COMET taxonomy. Data are summarised using descriptive statistics.
Results: Seventy-three eligible studies were identified: 27 controlled trials (randomised/ pseudo-randomised/ non-randomised) and 46 observational studies. Fortyfive studies (62% of included studies) reported on CGA in patients undergoing emergent orthopaedic/trauma surgery. A median of seven unique outcome measures were identified per study (IQR4-12) with length-of-stay (n=54/73, 74%) and mortality (In-hospital mortality n=31/73, 42%; 1-year mortality n=21/73, 29%; 1-month mortality n=19/73, 26%) reported most commonly. Domain mapping showed frequent reporting of outcomes evaluating healthcare resource utilisation (n=62/73, 85%) and postoperative complications (n=51/73, 70%), with under-representation of patient-reported or quality-of-life metrics (n=6/73, 8%). Additionally, few studies reported on the cost-effectiveness of perioperative CGA (n=8/73, 11%).
Conclusion: Our analysis shows heterogeneity in outcome measures in studies evaluating CGA-based perioperative medicine services. Consensus regarding core outcome measures is required.
Keywords: Perioperative medicine; Geriatric assessment; Outcome measures.
Introduction
Comprehensive Geriatric Assessment (CGA) is a multi-component, multidisciplinary intervention for older adults which utilises objective measures to holistically evaluate and optimise the medical, functional, social, and psychological components of an individual’s health [1]. This systematic intervention has demonstrated efficacy in improving clinical outcomes for older adults in both the inpatient and outpatient settings [2,3]. Notably, evidence from several previous randomised controlled trials and observational studies supports the incorporation of CGA into perioperative pathways for older surgical patients. This population are at high risk of postoperative geriatric syndromes, decompensation of co-morbid conditions, and functional deconditioning [4-6].
However, CGA is a complex intervention that requires specialist input from multiple healthcare professionals and often longitudinal intervention across several time points [7]. As a result, variation exists in the ability of centres to implement and deliver this intervention in the perioperative setting [8]. There is also variable delivery of perioperative CGA-based services across different surgical specialties [9]. To understand the barriers and enablers to the uptake of CGA-based perioperative services, and evaluate the clinical and cost-effectiveness of these services at scale across surgical subspecialties, multi-centre implementation-effectiveness trials are required.
Studies to address the above questions are hampered by a lack of consensus regarding outcome measures used in evaluating the complex intervention of CGA. Indeed, previous studies assessing CGA-based perioperative services have reported a wide range of outcomes measures [10]. This heterogeneity limits comparison between studies and creates difficulties for centres in selecting metrics to appraise the effectiveness of new perioperative services. The Core Outcome Measures in Effectiveness Trials (COMET) Initiative was established in 2010 to combat this heterogeneity by encouraging the development and utilisation of a Core Outcome Set (COS) for clinical trials [11]. An established COS for general perioperative and anaesthetic care has been published previously [12], but no recommended set of outcome measures for CGA-based perioperative medicine exists. Whilst an umbrella review has explored outcome measures used to evaluate the impact of CGA across healthcare settings [13], the findings were not specific to perioperative medicine.
This scoping review describes outcome measures used by studies evaluating the efficacy of CGA-based perioperative care compared with standard surgical care, maps these outcome measures to perioperative medicine core domains, and forms the first step in the generation of a COS for ongoing evaluation of CGA-based perioperative services. We aim to define a COS that can be used to describe the unique needs of the older surgical population, the holistic nature of CGA and the implementation of CGA-based perioperative services at scale (Figure 1).
Aim and objectives
Aim: To systematically identify and categorise outcome measures used in studies assessing the effectiveness of CGA-based perioperative medicine services for older adults undergoing surgery, when compared to routine perioperative care.
Objectives: To describe the outcome measures used to evaluate CGA-based perioperative services.
To describe the surgical specialties in which CGA-based perioperative services have been evaluated.
Methods
Reporting and registration
The protocol for this scoping review was decided a priori, in concordance with previously published methodology [14,15], and pre-registered on the Open Science Framework (https:// doi.org/10.17605/OSF.IO/5S9A8). Deviations from the initial protocol are described in Appendix S1 of the Supplementary Material. This scoping review is additionally reported according to the guidelines provided in the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR)’ checklist as shown in Appendix S2 of the Supplementary Material [16].
Information sources and search strategy
A systematic search of published literature was performed in Embase, MEDLINE, and Web of Science, on 26th April 2023. The search strategy for each database was designed by one author following consultation with a senior library assistant, and subsequently reviewed by two other authors with expertise in the field. An example search strategy from one online database is shown in Appendix S3 of the Supplementary Material. Searches were limited to articles published in English, and to studies published after the year 2000. The reference lists of previously published systematic reviews evaluating CGA-based perioperative medicine services were also reviewed to identify additional studies meeting the eligibility criteria.
Eligibility criteria
Population – older surgical patients: Eligible studies included older adults (aged >/= 65 years old) undergoing elective or emergency surgery. No restriction was imposed on the nature of the surgical procedure studied. The Centre for Perioperative Care delineates the perioperative period from ‘the moment of contemplation of surgery until full recovery’ [17]. This definition has been utilised throughout this review.
Intervention – CGA-based perioperative medicine
All included studies reported on the provision of perioperative care based on the principles of CGA as outlined by the British Geriatrics Society [1]. Care was delivered by a team involving at least one consultant geriatrician or geriatric medicine specialist nurse, and involved multi-domain assessment with interventions to optimise modifiable risk factors in the preoperative and/or postoperative period. Domains assessed during CGA included at least two of the following: physical, socioeconomic/ environmental, functional, mobility/ balance, psychological/ mental health, and medication review [1]. Studies evaluating assessments and interventions targeted at a single domain were excluded. Studies utilising CGA as a screening or risk stratification tool to predict postoperative outcomes were also excluded.
Comparator – routine surgical care
We included studies directly comparing CGA-based services with pre-existing, standard care for surgical patients at the home institution. This encompassed studies from institutions where a form of geriatric assessment, or a geriatric liaison service, had already been implemented within the surgical pathway, provided that the study directly compared this ‘standard’ model to the integration of a new CGA-based perioperative model. Only those outcome measures included in such studies which directly compared the CGA-based model to routine care were included in the analysis.
Study design
Studies reporting any experimental or quasi-experimental study design with at least 100 participants were eligible for inclusion, including randomised control trials, observational studies (retrospective and prospective) and results published from quality improvement projects. Literature reviews, systematic reviews, meta-analyses, and study protocols were excluded. Additionally, case reports, editorials and conference abstracts were excluded due to difficulties in ensuring fidelity to the principles of CGA. Smaller studies with fewer than 100 participants were also excluded as we sought to capture those outcome metrics which can be measured at a sufficiently large scale within future implementation-effectiveness trials.
A summary of the eligibility criteria for this scoping review is presented in Box 1.
Data screening
A web-based application, Rayyan [18], was used to collate studies, deduplicate (automatic and manual) and record exclusion/ inclusion decisions. Titles and abstracts were screened according to the inclusion/ exclusion criteria by two independent reviewers. Any study accepted by at least one reviewer at this initial screening stage was deemed suitable for progression to the next stage. Full texts of those studies identified by abstract/ title screening were subsequently assessed independently by two reviewers before confirming inclusion. Disagreements between reviewers following full-text review were resolved by discussion between both parties following unblinding.
Data items and extraction
Data extraction from the full texts of eligible studies was performed and collated in a pre-defined Microsoft Excel template (Supplementary File 1). Data points were extracted by one reviewer.
The following variables were extracted from each study:
• Authors.
• Year of publication.
• Study design/ methodology.
• Number of participants.
• Surgical specialty/ type of operation.
• Details of intervention.
• Details of comparator.
• Individual outcomes measures (recorded as close as possible to wording reported in each study without loss of meaning). Only outcome measures directly comparing CGA to standard care were extracted.
• Outcomes measurement tools (if reported).
• Time points for outcome measurement.
Risk of bias assessment
No formal assessment of study quality, or risk of bias, has been performed in keeping with our scoping review methodology, which aims to map, rather than evaluate, the previously published literature on perioperative CGA.
Data synthesis and analysis
Summary descriptive statistics analysing the design and affiliated surgical specialties of included studies are presented. Comparative outcome measures used in eligible studies were extracted verbatim, and subsequently standardised, based on the overarching concept to account for variation in phrasing between studies and allow identification of comparable, unique outcomes [19]. We then clustered our standardised outcome measures into core domains based on an adapted version of the taxonomy proposed by the COMET initiative [20], accounting for the unique features of CGA-based perioperative medicine and caring for older adults. Our categorisation system for these domains is shown in Box 2, which also depicts the associated COMET core areas (death, life impact, adverse events, resource usage). Where a specific outcome measure could be categorised into more than one domain, all applicable domains were assigned to the study.
Descriptive statistics were used to summarise the individual outcome measures and core domains reported in each study. Statistical analyses were performed using SPSS Statistics 29.0.2.0 and GraphPad Prism 10. Narrative synthesis has additionally been used to describe trends in the reporting of particular outcome domains. No formal meta-analysis has been conducted, in keeping with scoping review methodology.
Results
Study characteristics
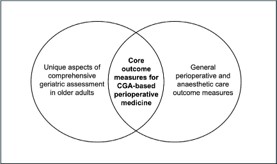
Our systematic search of three online databases, supplemented with citation searching from three previously published systematic reviews evaluating perioperative CGA, identified a total of 8,436 articles. Following de-duplication, the abstracts of 5,971 articles were screened for inclusion. The results of abstract and full-text screening are detailed in the PRISMA (Preferred Reporting Items for Systematic Reviews and MetaAnalyses) diagram in Figure 2, which also shows the reasons for article exclusion. Two-stage screening with independent reviewers resulted in the inclusion of 73 studies in the final analysis, which reported on a total of 65 participant cohorts (eight studies described post-hoc/ follow-up analyses on a previously studied cohort). Table S1 of the Supplementary Material contains a full reference list of included studies.
Date of publication
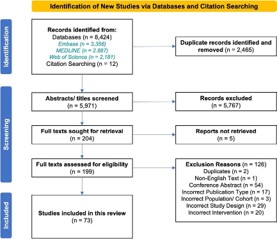
All included articles were published between 2001-2023. The distribution of publication years is shown in Figure 3a, which highlights the expansion in studies reporting on CGAbased perioperative medicine after 2015. The median year of publication was 2017, with an interquartile range of 2013-2020.
Study methodology
Of the 73 included articles, observational studies were the most common study type identified by our screening strategy (n=46/73, 63%) This included controlled before-and-after/ historically controlled studies (n=23/73, 32%), retrospective and prospective cohort studies (n=19/73, 26%), a case-control study (n=1/73, 1%), and population-level epidemiological studies (n=3/73, 4%). A total of 24 reports on Randomised Controlled Trials (RCT) were identified (33%) with one study describing a pseudo-randomised controlled trial (n=1/73, 1%). Additionally, two reports of non-randomised controlled trials were included (n=2/73, 3%). This distribution in study methodology is summarised in Figure 3b.
Participant numbers
The included studies had participant numbers ranging from 100 to 266,499 (this outlying large number of participants was included in one article describing a multilevel, multivariable population-based regression model across multiple elective, non-cardiac surgeries). The median number of participants was 279, with an interquartile range of 187-447.
Surgical specialty
As shown in Figure 3c, most identified studies evaluated the integration of CGA-based perioperative services into pathways for older adults undergoing orthopaedic/ trauma surgery (n=47/73, 64%), particularly those undergoing emergency repair of a hip fracture (n=45/73, 62%). 13 studies included participants undergoing upper/ lower gastrointestinal surgery (n=13/73, 18%), of which the majority reported on colorectal surgical procedures. The next most common surgical specialities studied were vascular surgery (n=6/73, 8%) and surgical oncology (n=4/73, 5%), with only single studies reporting on cardiac and urological procedures. Additionally, 1 large population-level study reported across multiple elective, non-cardiac surgical specialities including orthopaedic, vascular, gastrointestinal, hepatobiliary, thoracic and urological surgery.
A full overview of the characteristics of studies included in this analysis is shown in Table S2 of the Supplementary Material.
Reporting of outcome measures
Following the extraction of verbatim outcome measures, individual terms were standardised to allow appropriate comparisons between studies. This homogenisation process resulted in the number of comparative outcome measures per study ranging from one – 30. The median number of unique outcome measures per study was seven (interquartile range four – 12). In total, 165 unique outcomes were identified. The most frequently reported standardised outcomes across studies are shown in Table 1. Common outcome measures included the length of acute admission (n=54/73, 74%), the need for re-admission following discharge (n=33/74, 45%), and death by any cause (n=47/73, 64%). Notably, studies showed heterogeneity in the time points at which mortality was reported (with several studies reporting mortality at multiple time points). In-hospital mortality was reported most frequently (n=31/73, 42%), followed by one-year mortality (n=21/73, 29%) and one-month mortality (n=19/73, 26%).
Conversely, of the 165 individual outcome measures collated from our search, 81 outcomes were reported on only one occasion (within one study). The singular reporting of these outcomes prevents any comparison of such metrics between studies. A complete list of reported outcome measures is shown in Table S3 of the Supplementary Material.
Domain mapping and reporting
Mapping of extracted outcomes onto core domains adapted from COMET taxonomy was performed to better appreciate the patterns of reporting on issues specific to perioperative care of older adults (Box 2; Mortality, Perioperative Optimisation, Geriatric Syndromes, Patient and Family/Carer Reported Outcome Measures, Postoperative Complications/ Morbidity, Inpatient and Outpatient Healthcare Usage, Care Requirements and Hospital Discharge, Economic Evaluation). This domain mapping process is shown for a representative example in Table S4 of the Supplementary Material. The number of studies with outcomes addressing each core domain is shown in Figure 4.
Healthcare resource usage (both during the acute surgical admission and during outpatient care) was commonly reported (n=62/73, 85%). Outcomes in this domain included length of stay (n=54/73, 74%), hospital re-admissions (n=33/74, 45%), time to surgery from presentation (n=22/73, 30%), number of referrals/ assessments by external medical specialties (n=6/73, 8%), intensive care unit admissions (n=6/73, 8%), emergency department attendances following discharge (n=5, 7%), and postoperative inpatient/ bed-based rehabilitation (n=4/73, 5%).
After healthcare resource usage metrics, the next most common domains were postoperative complications/ morbidity (n=51/73, 70%) and mortality (n=47/73, 64%). Many different postoperative complications were prioritised across different studies, including cardiovascular events (e.g., acute coronary syndromes/ arrhythmias/ cardiac failure, n=19/73, 26%), respiratory issues (e.g., infection/ pulmonary congestion/ exacerbation of chronic airways disease, n=18/73, 25%) and renal derangement (acute kidney injury, n=14/73, 19%). Fifteen studies reported a summative total of postoperative complications in addition to specific pathologies.
All included studies delivered multidomain CGA with oversight from a consultant geriatrician or specialist nurse; as a result, measures relating to common postoperative geriatric syndromes and assessment of patient mobility/ cognition/ functional status were commonplace (n=46/73, 63%). Delirium was the most frequently reported geriatric syndrome (n=26/73, 26%), followed by inpatient falls (n=12/73, 16%) and pressure associated skin damage (n=11/73, 15%). Postoperative mobility and ambulation were reported using a variety of outcome measures. These included the proportion of patients independent in ambulation/ transfers postoperatively (n=5/73, 7%), the requirement for a new walking aid postoperatively (n=3/73, 4%), Timed-Up-And-Go (TUAG, n=2/73, 3%), Short Physical Performance Battery (SPPB, n=3/73, 4%), and the number of days from surgery to ambulation (n=2/73, 3%).
Similarly, the assessment of functional status varied between studies. Several batteries providing quantitation of activities-of daily-living were reported, including the Instrumental Activities-of-Daily-Living scale (IADL scale, n=4/73, 5%), the Chinese Barthel Index score (CBI score, n=4/73, 5%) and the Katz Activities-of-Daily-Living index (Katz ADL index, n=3/73, 4%). More commonly, studies simply reported whether a patient’s requirement for carer support had changed at the point of discharge compared with admission (n=9/73, 12%). Notably, this outcome measure overlapped with another of our core domains focusing on patient care requirements and hospital discharge, a key consideration for hospitalised older adults. This domain was reported in 32 of our 73 included studies (44%) and included additional measures such as the patient’s discharge destination after acute hospitalisation (n=26/73, 36%) and the prevalence of delays in discharge from the hospital (n=4/73, 5%).
Cognition was assessed less frequently than mobility and functional status, with the Mini-Mental State Exam (MMSE, n=5/73, 7%), the Clinical Dementia Rating Scale (n=2/73, 3%), the Informant-Questionnaire-on-Cognitive-Decline-in-the-Elderly (IQCODE, n=1/73, 1%), and the Consortium-to-Establisha-Registry-for-Alzheimer’s-Disease (CERAD) 10-Words-Test (n=1/73, 1%) all reported.
Outcomes examining the role of the geriatric medicine team in perioperative optimisation were reported in 21 of our 73 included studies (29%). These outcomes related to the management of several comorbid medical conditions including osteoporosis (n=5/73, 7%), depression (n=1/73, 1%), anaemia (n=1/73, 1%) and secondary prevention of atherosclerotic disease (n=1/73, 1%). One study also reported on medication rationalisation following geriatric assessment. Shared decisionmaking discussions were occasionally reported, with a particular focus on the decision to proceed with surgical or non-surgical management (n=5/73, 7%).
The least commonly used outcome domains were patient and caregiver-reported outcome measures (n=6/73, 8%), and economic evaluation (n=8/73, 11%). Of the small number of studies with patient-reported outcome measures (PROMS) and quality-of-life metrics, the SF-36 health survey was most frequently used (n=4/73, 5%) followed by EQ-5D instruments (n=3/73, 4%). Only one study included outcome measures specifically relating to caregivers/ family members (42-Item Agitation Management Self-Efficacy Scale for caregivers/ 17-Item Chinese-Version Caregiver Competence Scale). Of the studies which described the cost-effectiveness of implementing a perioperative CGA service, most reported on the per-patient cost of the inpatient hospital stay (n=5/73, 7%). Quality-adjusted life-years (QALYs) were also calculated in two studies, with one reporting the incremental net QALY benefit of CGA compared to standard care, and the other describing the difference in mean QALYs relative to the difference in mean cost.
The median number of core outcome domains utilised per study was four (interquartile range three – five).

Table 1: Table showing the most frequently reported outcome measures across included studies, following the standardisation of terminology. Values show the number of studies reporting each metric.
| Outcome measure | Frequency (n=73) |
|---|---|
| Length of stay | 54 |
| Mortality | 47 |
| In-hospital mortality | 31 |
| 1-year mortality | 21 |
| 1-month mortality | 19 |
| Hospital re-admission after discharge | 33 |
| Complications – delirium | 26 |
| Discharge destination after acute hospitalisation | 26 |
| Time to surgery | 22 |
| Complications – Cardiovascular | 19 |
| Complications – Respiratory | 18 |
| Complications – Total (undifferentiated) | 15 |
| Complications – Renal/Acute Kidney Injury (AKI) | 14 |
| Complications – Falls | 12 |
| Complications – Urinary Tract Infection (UTI) | 11 |
| Complications – Pressure ulcer | 11 |
| Complications – Haematological/Anaemia/Bleeding | 10 |
| Complications – Venous Thromboembolism (VTE) | 10 |


Discussion
We identified 73 studies, reporting on 65 patient cohorts, which have evaluated the effectiveness of integrating multidomain geriatric assessment into the surgical pathways for older adults undergoing elective and emergency surgery. We have collated the 165 unique outcome measures prioritised by previous research groups, providing an informative overview of those metrics which have historically been deemed most relevant to studies of CGA-based perioperative medicine. Moreover, by mapping these outcomes into core domains, we have identified several important trends in the existing literature. First, the role of geriatric assessment in surgical care has been most widely studied in orthopaedic surgical populations, which is unsurprising given the prevalence of frailty and multi-morbidity in this group of patients [21,22]. While colorectal and vascular surgery patients have also been included in several studies, the relative proportion of studies remains low. Second, patientreported outcome measures are described infrequently when compared to clinician-reported, quantitative measures. This is despite the reported importance of quality-of-life metrics for both older adults receiving acute care [23,24], and for healthcare staff working within geriatric medicine [25,26]. Similarly, few studies consider the health economics of implementing a new perioperative medicine service, and those that report cost-effectiveness use disparate reporting measures.
There is also a lack of consensus in the literature regarding the scoring systems that should be used to assess key CGA domains such as mobility, functional status, and cognition. Additionally, reporting on the role of CGA in optimising co-morbid medical issues and the resultant effect on an individual’s overall health is often neglected when compared with metrics relating directly to the presenting surgical pathology, such as mortality and in-hospital complications. This may account for some of the difficulties encountered by previous centres in demonstrating the clinical effectiveness of perioperative CGA [8].
This review offers key insights into the heterogeneity which exists in the patient populations and outcome measures used to evaluate CGA-based perioperative medicine services. There are also several limitations to this review. No assessment of study quality was performed, in keeping with our scoping review methodology. Additionally, no synthesis of evidence on the effectiveness of CGA-based services across specialties was conducted. Similarly, this review does not report on variations in how CGA was delivered at different centres, which could be a beneficial output for understanding the divergent ability of hospital services to implement perioperative CGA. Finally, standardisation of study terminology to allow more effective comparisons between studies, and a more succinct synopsis of the published evidence, will have invariably led to the loss of some more subtle distinctions between chosen outcome measures [19].
The results of this scoping review and outcome mapping will inform the development of a standardised core outcome set for international use in studies of perioperative CGA-based services. Establishing this core outcome set will require further input from clinical and academic experts, patients, and the public using a modified Delphi or nominal group technique for iterative refinement.
Conclusion
In summary, this scoping review identifies 73 studies, reporting on 65 patient cohorts, utilising 165 unique outcome measures to evaluate the effectiveness of CGA-based perioperative medicine for older adults. The insights gained from collating and categorising these outcomes will now be refined with input from experts and patient groups to reach an agreed core outcome set. This will promote standardisation and enhance the validity of future studies evaluating the implementation of CGAbased perioperative services.
Declarations
Acknowledgements/funding: No external funding and no competing interests declared.
Conflicts of interest: Authors have no conflicts of interest to declare.
References
- British Geriatrics Society. Comprehensive geriatric assessment toolkit for primary care practitioners. 2019. (accessed 25/03/2025)
- Ellis G, Gardner M, Tsiachristas A, et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. 2017; 9: Cd006211.
- Yen P-C, Lo Y-T, Lai C-C, et al. Effectiveness of outpatient geriatric evaluation and management intervention on survival and nursing home admission: A systematic review and meta-analysis of randomized controlled trials. BMC Geriatrics. 2023; 23: 414.
- Tan H-J, Saliba D, Kwan L, Moore AA, Litwin MS. Burden of geriatric events among older adults undergoing major cancer surgery. J Clin Oncol. 2016; 34: 1231–8.
- Partridge JSL, Harari D, Dhesi JK. Frailty in the older surgical patient: A review. Age Ageing. 2012; 41: 142–7.
- McRae PJ, Walker PJ, Peel NM, et al. Frailty and geriatric syndromes in vascular surgical ward patients. Ann Vasc Surg. 2016; 35: 9–18.
- Sum G, Nicholas SO, Nai ZL, Ding YY, Tan WS. Health outcomes and implementation barriers and facilitators of comprehensive geriatric assessment in community settings: A systematic integrative review. BMC Geriatrics. 2022; 22: 379.
- Joughin AL, Partridge JSL, O’Halloran T, Dhesi JK. Where are we now in perioperative medicine? Results from a repeated UK survey of geriatric medicine delivered services for older people. Age Ageing. 2019; 48: 458–62.
- Miller RL, Barnes JD, Mouton R, Braude P, Hinchliffe R. Comprehensive geriatric assessment (CGA) in perioperative care: A systematic review of a complex intervention. BMJ Open. 2022; 12.
- Eamer G, Taheri A, Chen SS, et al. Comprehensive geriatric assessment for older people admitted to a surgical service. Cochrane Database Syst Rev. 2018; 1: Cd012485.
- Williamson PR, Altman DG, Blazeby JM, Clarke M, Gargon E. The COMET (core outcome measures in effectiveness trials) initiative. Trials. 2011; 12: A70.
- Boney O, Moonesinghe SR, Myles PS, et al. Core outcome measures for perioperative and anaesthetic care (COMPAC): A modified Delphi process to develop a core outcome set for trials in perioperative care and anaesthesia. Br J Anaesth. 2022; 128: 174–85.
- Veronese N, Custodero C, Demurtas J, et al. Comprehensive geriatric assessment in older people: An umbrella review of health outcomes. Age Ageing. 2022; 51.
- Arksey H, O’Malley L. Scoping studies: Towards a methodological framework. Int J Soc Res Methodol. 2005; 8: 19–32.
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: Advancing the methodology. Implement Sci. 2010; 5: 69.
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-SCR): Checklist and explanation. Ann Intern Med. 2018; 169: 467–73.
- Centre for Perioperative Care. https://www.cpoc.org.uk/about- cpoc/what-perioperative-care (accessed)
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan— a web and mobile app for systematic reviews. Syst Rev. 2016; 5: 210.
- Young AE, Brookes ST, Avery KNL, Davies A, Metcalfe C, Blazeby JM. A systematic review of core outcome set development studies demonstrates difficulties in defining unique outcomes. J Clin Epidemiol. 2019; 115: 14–24.
- Dodd S, Clarke M, Becker L, Mavergames C, Fish R, Williamson PR. A taxonomy has been developed for outcomes in medical research to help improve knowledge discovery. J Clin Epidemiol. 2018; 96: 84–92.
- Gleason LJ, Benton EA, Alvarez-Nebreda ML, Weaver MJ, Harris MB, Javedan H. FRAIL questionnaire screening tool and shortterm outcomes in geriatric fracture patients. J Am Med Dir Assoc. 2017; 18: 1082–6.
- Xi S, Wu Z, Cui J, Yin S, Xi S, Liu C. Association between frailty, as measured by the FRAIL scale, and 1-year mortality in older patients undergoing hip fracture surgery. BMC Geriatrics. 2025; 25: 65.
- Phelps K, Regen E, van Oppen JD, et al. What are the goals of care for older people living with frailty when they access urgent care? Are those goals attained? A qualitative view of patient and carer perspectives. Int Emerg Nurs. 2022; 63: 101189.
- Dresden SM, McCarthy DM, Engel KG, Courtney DM. Perceptions and expectations of health-related quality of life among geriatric patients seeking emergency care: A qualitative study. BMC Geriatrics. 2019; 19: 209.
- Conroy SP, van Oppen JD. Are we measuring what matters to older people? The Lancet Healthy Longevity. 2023; 4: e354–6.
- Welch C, Wilson D, Sayer AA, et al. Development of a UK core dataset for geriatric medicine research: A position statement and results from a Delphi consensus process. BMC Geriatrics. 2023; 23: 168.