Volume 1, Issue 2
Article Type: Research Article
Rotator cuff tear related shoulder osteoarthritis and vitamin C: A brief review of the literature
Ray Marks*
Department of Research, Osteoarthritis Research Center, Box 5B, Thornhill, ONT L3T 5H3, Canada
*Corresponding author: Ray Marks
OARC Clinical Research and Education Director, Ontario L3T
5H3, Canada.
Tel: +1-647-968-2725; Email ID: Dr.RayMarks@osteoarthritisresearchcenter.com; rm226@columbia.edu
Received: Jul 24, 2025
Accepted: Aug 13, 2025
Published Online: Aug 19, 2025
Journal: Annals of Pediatrics and Neonatal Care
Copyright: Marks R et al. © All rights are reserved
Citation: Marks R. Rotator cuff tear related shoulder osteoarthritis and vitamin C: A brief review of the literature. Ann Gerontol Geriatr Res. 2025; 1(2): 1017.
Abstract
Osteoarthritis, the most prevalent joint disease remains relatively impervious to a desired reversal of its progressive impact on function and life quality in the older adult population. Moreover, even if available, drug treatments may not be indicated, efficacious, or safe and commonly fail to alter the disease directly including joint tissue damage, inflammation, and muscle pathology. At the shoulder, osteoarthritis is frequently subject to debilitating upper arm mobility dysfunction especially in the face of persistent rotator cuff tears. The question arises as to whether antioxidants such as vitamin C may prove helpful here, especially in fostering tendon healing, and even if not, protecting vulnerable older adults from excess pain, suffering and joint destruction. Building on prior in-depth overviews capturing almost all data on this topic prior to mid-2024, here we present a synthesis of some newer data on this topic published since 2024 that discuss a role for vitamin C as one non drug mechanism that may help mitigate the severity of shoulder osteoarthritis and any associated supportive tissue damage, even in later life. We conclude this issue is promising but lacks validity, thus should be intently explored to prevent overlooking a promising non-narcotic osteoarthritis pain and free radical reduction source, as well as possible soft tissue and shoulder stabilizing joint tissues.
Keywords: Aging; Cartilage; Joint; Osteoarthritis; Pain; Rotator Cuff; Shoulder; Tendon; Vitamin C.
Introduction
Osteoarthritis a widespread highly disabling joint disease affecting many older adults remains an immensely costly public health challenge with few means of mitigation [1]. A commonly progressive disease that affects multiple joint tissues, such as those at the shoulder, including the cartilage shock absorbing tissue lining the shoulder and those vital tendons that attach the shoulder muscles and move and stabilize the joint, thereby eliciting progressive dysfunction of the upper arm, immense pain and stiffness or instability. Unfortunately, with no universally agreed upon prevention or intervention approach a pattern of increasing disability, and one that encompasses limited function of the upper limb may emerge and render self-care in the most affected cases, highly challenging at best.
Severely impacting the goal of independent living, the ability of the older adult with shoulder osteoarthritis to attain their lifes’ goals and others may be jeopardized. They may become anxious and depressed and unwilling to move the arm even if help is provided, for example in dressing. At the same time and with no respite, osteoarthritis, may be deemed to set the stage that can foster a high presence of negative biochemical pro-oxidant intracellular chemical processes termed Reactive Oxygen Species (ROS). This set of processes which are correlated with increasing age, are implicated in chronic degenerative diseases such as osteoarthritis and are of great import to mitigate. At the aging shoulder joint the stimulation and activation of reactive oxygen species can set the stage for the ongoing degradation of associated cell membranes, tissue biology and structures such as tendons. Their actions alone may serve to induce an unstoppable degree of joint attrition, plus joint dysfunction, stiffness, pain, signs of chronic joint inflammation, muscle mass declines, muscle fat encroachment, and multiple functional limitations plus cumulative degrees of structural damage [2].
Unfortunately, while many pharmacologic and surgical approaches prevail, many of these may be unsafe for an older adult to pursue. In this regard, vitamin C an essential nutrient with immune boosting and antioxidant properties appears to hold some considerable promise as an adjunctive preventive and remedial strategy in older adults and in cases suffering shoulder osteoarthritis [3,4].
Indeed, recent studies reveal its presence may have potential influences in enhancing cartilage regeneration processes, muscle function, and repairing tendons [5-7]. Other potentially noteworthy actions are its ability to modulate multiple neural functions that can elicit neuropathic pain. Other data show it has a crucial role to play in collagen synthesis, stress control and health, in general [5-8].
Applied in the realm of osteoarthritis vitamin C supplements appear of high relevance in efforts to minimize the magnitude and intensity of any prevailing joint destruction processes and pain that emerges over time. Alternately, its optimal presence and potentially favorable wound healing properties and others may help prevent associated or excess cartilage tissue damage, while fostering vitally important collagen synthesis, as well as tendon healing [7]. Moreover, the fact that oxidative damage is a potential remediable osteoarthritis moderator, speaks to why vitamin C, known to have specific antioxidant properties, can potentially counter the production of damaging pain provoking free radicals that would otherwise have multiple negative local joints as structural, immunological, and cognitive implications for the sufferer [8,9].
In the face of few safe cost-effective options and escalating aging populations who may suffer from shoulder osteoarthritis, this array of possibility benefits attributed to the presence of adequate vitamin C levels seems especially important to explore as it may avert the higher doses of unsafe medications that may otherwise be needed over time. In some cases, too drugs may prove toxic to joint tissues as well as collagen production, essential for tendon repair, or have fatal side effects, for example if osteoarthritis pain relief is dependent on narcotics. Other data reveal some anti-inflammatory drugs can indeed hasten, rather than slow the disease process, and do not always reduce pain [10]. In addition, some recently tested biologics that are quite well supported in theory, have failed to show promise in slowing the rate of osteoarthritis joint space narrowing. On the other hand, a strategy that can favorably influence the structural and functional properties of the cartilage lining of both a healthy as well as an osteoarthritis affected joint, and its surrounding muscles, tendons, nerve supply, and bone in a positive way, may both safeguard or help to foster overall physical ability, other data reveal some anti-inflammatory drugs can indeed hasten, rather than slow the disease process, and do not always reduce pain [10] or foster upper arm functions, for example if the shoulder is ‘frozen’ or unstable, both states often being the cause of immense suffering in all spheres of life, even the ability to sleep soundly.
The reason for focusing on vitamin C is not that it is a ‘cure all’, but recent investigations on the biochemical pathways that preside post musculoskeletal injury-point to a strong cause of vitamin C deficiency in influencing shoulder osteoarthritis chronicity and tendon attrition [12]. In addition, its deficiency can be expected to negatively impact overall health, plus cartilage, and bone repair [9], and hamper attainment of desirable levels of skeletal muscle mass [13]. Although many cases of shoulder osteoarthritis in young adults arise from trauma, it is the older adult with often no known cause who has fewer treatment options or adaptive regeneration capacities.
Aims
This mini review follows others that have been conducted over time so as to update the extent of support for the idea that vitamin C, an established mediator of tissue biology, growth, and development with powerful antioxidant and anti-inflammatory properties may be an influential modifiable factor in the context of efforts to minimize, modulate or mediate osteoarthritis pain in general, and more specifically at the shoulder joint where the rotator cuff tendons are highly problematic to treat or repair especially in the older adult. A secondary aim was to establish whether further research is warranted in this realm given the burden of the disease alone and the purported role vitamin C plays in collagen synthesis and many key enzymatic essential life-affirming biological, metabolic, genetic, molecular, and neurological processes implicated in osteoarthritis and tendon. Region specific data appear of high import here as opposed to more general facts, and the shoulder, a non-weight bearing joint and its osteoarthritis disease trajectory may not be analogous to that occurring at one of the weight bearing joints. Vitamin C is a possible low-cost alternative to shoulder surgery, poor surgical outcomes, neuropathic pain, progressive tendinopathy pathology and health costs thus favored by those who have socioeconomic hardships and disabling functional abilities that limit exercise participation and access to a provider.
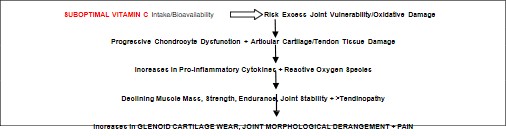
Tested is the idea that the presence of adequate vitamin C has a distinct bearing on directing potential cartilage healing opportunities in osteoarthritis, as well as the pain experience and in shoulder osteoarthritis may influence the healing potential of the surrounding soft tissues and joint stabilizers, but fail to preserve the older adult shoulder osteoarthritis if insufficient as outlined in Figure 1.
Methods
To achieve these abovementioned review aims, we elected to build on an extensive general review of available documents housed on PUBMED between January 2024-August 2025 using the key terms Vitamin C and Osteoarthritis/Rotator Cuff/ Shoulder/Tendon. More specifically, PUBMED the predominant medically oriented website was used to provide a global overview of vitamin C related osteoarthritis and more specifically shoulder osteoarthritis research pertaining to the problem of rotator cuff tears that can foster immense disability or arise as a consequence of chronic injury and one of limited reparative potential worsened by age. The currently published works listed were duly scanned for salience by the author and the selection process was made on the basis of time and relevance to all stages of possible shoulder lesion injuries and osteoarthritis shoulder joint degeneration. Readers can learn more by exploring the current cited general reports as well as some prior reports [eg., Maxfield [9], Stanborough et al. [11]; and Marks [14,15].
Results
As of August 1 2025, only a small number of relevant studies on osteoarthritis as a whole, and especially that at the shoulder, where it is common, were found. Even when combined with prior data these current reports remain challenging to unify and even in comparable studies no firm agreement in any sphere has emerged to date. The limited numbers of reports in this regard is unlike those for the immense volumes of that on hip and knee osteoarthritis focus mainly on surgical methods and outcomes, and make it generally impossible to discern a role for non-pharmacologic approaches. Difficult to aggregate in any sphere to date with confidence is however not only due to their scarcity, but their small samples, diversity, questionable measurement approaches and unknown measurement properties.
Those that have emerged in the lab or through tissue sampling, imagery and secondary subjective oriented reports may not offer insights or replicate human osteoarthritis as it occurs at the shoulder in the older person at all accurately.
Moreover, to date, no consistent aspect of vitamin C is addressed, and its mode or terminology is quite inconsistent and appears to be arbitrary. For example, some groups focus on vitamin C deficiency effects, others focus on its possible supplementary effects, others on its anti-inflammatory effects, and others on its pro-oxidant effects [12-17]. Other data within a study reveal a vegetable intake and a diet that contains vitamin C appeared to be helpful in averting knee osteoarthritis risk, but not at high consumption levels [18].
Unfortunately, even if vitamin C can yield cartilage-associated protective influences in the lab [19-22], once joint destruction has commenced, a belief it is not possible to repair cartilage prevails, thus reducing the motivation possibly for study and raising further challenges in identifying precisely what might work to foster daily pain free function and why. Moreover, whether instruments and outcomes reported in current research reports are both reliable and valid and sensitive to change is also hard to ascertain, especially where data are studied from a perspective of patient derived estimates dependent on memory or food recall.
Whether supplement usage, quality and consistency is a robust indicator of vitamin C sufficiency in its own right must also await verification as must any clinically meaningful association between subjective measures of pain and vitamin C in shoulder osteoarthritis where cognitive pain pathways and responses may differ from that of the hip, hand, spine, or knee.
What is clear is that over time a substantive body of data tends to show that vitamin C has important antioxidant properties that can counter inflammation-a major pain producer at the shoulder joint-as well as serving as a co-factor in for numerous biochemical reactions involved in the synthesis and assembly of cartilage collagen, and its matrix [23]. In addition, its affinity to exert chondroprotective and/or cartilage tissue regenerative effects [20-22] and the maintenance of skeletal muscle functions [24,25] are of potential high significance.
Vitamin C may also mediate those aspects of the entire diseased joint that induce disability such as the structural features of joint ligaments, tendons, and bone quality and cartilage tissue. Its presence may well foster the rate of post orthopedic surgical recovery processes [26,27] that is the mainstay of shoulder osteoarthritis treatments. More specifically, when present at desired levels, vitamin C may render favorable associated outcome effects on bone production, soft tissue injury sites, pain, tendon and wound and fracture healing among other influential factors [26-30] such as its ability to lower post exercise muscle soreness levels [34] and a possibility of shoulder muscle atrophy [25].
Indeed, Chiu et al. [31] argue that these aforementioned vitamin C joint interaction observations while not universal are worthy of exploration, and may prevail even at low doses and in the face of due joint damage. By contrast, when deficient a situation arises that may foster the production of damaging cartilage chondrocyte enzymes, and ROS-injury provoking that has an adverse extracellular cartilage matrix breakdown impact [32]. Another body of data show however, an improved chondrocyte viability and proliferation and possible regeneration in the presence of adequate plasma vitamin C levels [32]. Another favorable observation is that vitamin C may aid or reduce oxidative stress at and within the shoulder rotator cuff tendon repair site, it may decrease pain, accelerate healing [33,35,36] plus articular cartilage tissue viability, while possibly allowing for a decreasing analgesic need, and thereby eliciting multiple functional as well as psychological benefits. Indeed, a recent report shows drug delivery of vitamin C via bioactive nano-magnetic particles in conjunction with a compound termed dexamethasone does tend to yield cartilage chondroprotective benefits that could alleviate shoulder osteoarthritis symptoms and repair as well as any shoulder tendon lesions and should duly explored [37,38]. Other benfits of vitamin C supplementation as applied to shoulder arthritis are summarized in Table 1.
Table 1: Selected data highlighting some possible clinically relevant benefits of attaining and maintaining optimal daily vitamin C levels in older adults suffering from shoulder osteoarthritis and rotator cuff tears, while avoiding excess disease and damage manifestations.
| Groups | Noteworthy findings |
|---|---|
| Ali et al. [17] | Vitamin C may mitigate arthritis inflammation |
| Burger et al. [39] | Vitamin C may attenuate osteoblast aging in those with osteoarthritis |
| Burton and McCormack [40] | Vitamin C may mitigate tendinopathy extent and inflammation |
| Chiu et al. [31] | Possesses multiple capacities for preventing or retarding osteoarthritis progress |
| D’Aniello et al. [41] | Regulates extracellular matrix/collagen homeostasis |
| DePhillipo et al. [12] | Can accelerate fracture healing |
| Increases collagen Type I synthesis | |
| Reduces oxidative stress parameters | |
| Hosseini et al. [28] | May reduce blood loss post-surgery |
| Huang et al. [42] | May have anti-inflammatory effects |
| May help improve cartilage matrix deposition | |
| Liao et al. [43] | May slow osteoarthritis progression in traumatically induced osteoarthritis |
| Qamar et al. [44] | Vitamin C enhance bone health and tendon healing |
| Surapaneni et al. [45] | It appears low vitamin C and excess oxidative stress impact osteoarthritis |
| Tang et al. [5] | Vitamin C reduces oxidative stress and inflammatory muscle responses in the realm of postoperative care |
| Yamamoto et al. [4] | May slow cartilage degeneration |
As well, findings of positive associations, of both dietary and circulating vitamin C with measures of skeletal muscle mass in middleand older-aged men and women, suggests that dietary vitamin C intake may be useful for reducing age-related muscle loss and associated issues related to collagen deficits in support tissues that may impact shoulder tendon repair and allow for more optimal surgical and conservative outcome expectations [30, 47-50].
Discussion
Osteoarthritis, a highly disabling joint disease and one where any form of palliative or reparative treatment that can safely reduce pain, would be highly prized, remains largely dependent on an array of pharmacologic and/or surgical interventions of varying degrees of efficacy and effectiveness with respect to the damaged or degraded shoulder joint. In this regard, despite considerable background research on the importance of overall health as a scaffold for preventing joint injury and fostering recovery from shoulder trauma and arthritis, and knowledge vitamin C is of key related importance plus an essential vitamin with diverse biologic influences [61] designed to minimize oxidative stresses that are injurious, very little has been forthcoming in the realm of applying vitamin C associated research towards understanding shoulder osteoarthritis pain and its possible reduction or prevention in the older adult population. Specifically, in terms of its impacts on daily living alone, and its relentless presence at night, more study of this arthritis condition where the pathology is not uniform and may leave sizeable numbers of aging adults more infirm than not is desirable.
Until then, despite a reasonably strong underlying rationale for believing that vitamin C is tentatively important for purposes of ensuring optimal joint health, and that older persons with or without osteoarthritis may be at risk for either a reduced ability to take up vitamin C or have a greater need for this vitamin than those who are not subject to inflammatory joint changes, the possibility that suboptimal vitamin C levels are related in some way to the presence of osteoarthritis pain and its severity and extent, and which is poorly studied, when compared to other topic areas concerning osteoarthritis pathogenesis and mitigation, more research of the older adult situation is indicated. Reflecting a patchwork of interesting studies but with no seemingly consistent underlying hypothesis, shoulder osteoarthritis in particular is very poorly studied in the non-invasive disease management realm and where more often than not the tendons attaching key muscles to the shoulder joint surface are torn and do not repair to any degree and may mar surgical as well as conservative success. Identifying and studying cellular and molecular levels of vitamin C and cartilage cellular impacts and their ability to foster muscle regeneration is still in its early research phases but will likely offer great promise.
Moreover, multiple preclinical studies strongly support the possibility of vitamin C as an adjunct for alleviating, minimizing, ameliorating, or reversing osteoarthritis cartilage damage, as well as having the ability to prevent the rate of osteoarthritis progression, including decreases in cell death and the expression of damaging pro-inflammatory cytokines and excess skeletal muscle atrophy [51].
However, this realm of investigation appears to warrant attention, for example, many studies examone combinations of vitamin C and other modes of intervention, thus what works and why cannot be readily discerned. Almost all current researchers are however unified in calling for more carefully designed efforts to address documented design shortcomings in promising studies and to thereby foster the ability to resolve the presently divergent viewpoints concerning any clinically relevant or efficacy associated impacts as well as the safety of various vitamin C doses that may affect osteoarthritis pathology and pain. In particular, prospective well controlled research designs are imperative, as are salient research questions and methods of inquiry using well defined and stringent measures, such as plasma level vitamin C assays plus structural measures at regular intervals.
Careful attention to assessing dose concentration relationships between vitamin C supplements, with and without any dietary sources, and medications that may impede vitamin C anabolic processes, and pain as well as functional correlates of various degrees of shoulder osteoarthritis can also help ensure that clinically meaningful relationships that emerge are robust.
In the interim, what we do know is that vitamin C is clearly an essential co-factor for fostering normal growth, and collagen synthesis, including collagen X [52], a major structural element of articular cartilage, and its surrounding tissues [53], as well as for other vital physiological chondrocyte, and bone cell functions [54]. It also appears deficient vitamin C levels are associated with pain provoking inflammation that often accompanies osteoarthritis [43]. There are also vitamin C transporter deficiencies that have the potential to markedly impact cartilage cell metabolism as well as cartilage collagen production, matrix formation and assembly, significantly and adversely that could explain osteoarthritis pain modulation challenges to some degree [55]. Vitamin C presence does however appear to be accompanied by improved pain scores, while helping subjects achieve better functional gains, shoulder osteoarthritis muscle and bone health [56,57].
Moreover, surgery for osteoarthritis or joint injuries may be optimized [58] and its potential to ameliorate sarcopenia a key shoulder arthritis determinant has been discussed as well [61]. It is also possible that although Joseph et al. [56] discount any vitamin C impact on osteoarthritis, its efficacy as an osteoarthritis protective factors has not been revealed uniformly and examined meticulously and comprehensively so as to rule out competing factors. Although often discussed, the role of suboptimal or noxious vitamin C supplementary doses, potentially unreliable assessments, omitted assessments, and the statistical problems of applying aggregated data from limited albeit diverse samples as recorded retrospectively or on a single occasion remains.
It is possible too that more attention to the notion that implies the presence of a persistent vitamin C deficiency is a potentially debilitating health factor that may inadvertently raise the risk for osteoarthritis joint damage is marred by the inability to currently estimate its influence in osteoarthritis risk and progression through retrospective modeling of data as far back as 2007 that may not focus on the older adult masks vitamin C as a determinant of high possible relevance in the context of older shoulder osteoarthritis cases accurately thus leading to a dismissal of its possible actual and significant effects [62], and those that occur indirectly and retard its recovery potential at all stages, including any post trauma stage.
Our limitation in what we have surveyed and analyzed for trends may play a confusing role, however, after surveying more than 225 related papers in 2018 and 2024 [14,15] and another 70+ since then in this report, wherein most were located in the world’s leading data base of PUBMED-deemed reliable and peer reviewedit appears safe to propose that persistent vitamin C deficits appear to have the potential to accelerate or magnify the risk of musculoskeletal injury and any subsequent joint pain such as that occurring in most older adults suffering from osteoarthritis, as well as possibly influencing osteoarthritis risk [63] and tendon healing. It may also be that an individual struggling with painful osteoarthritis who is under stress is particularly vulnerable to more pain and degrees of joint damage and has an increasing need for long-term vitamin C supplementation to minimize health challenges that can perpetuate a state of debility and provoke ROS-injury if this factor is ignored [65].
In sum, there appears to be a valid need to generate more insight into how vitamin C may be an important readily available low-cost osteoarthritis pathogenic and healing mediator. In particular, researching the association of vitamin C levels among distinctive osteoarthritis sub-groups such as cases with shoulder osteoarthritis may prove especially insightful. After that, meticulously and rigorously designed studies to rule out competing hypotheses, and to avoid undesirable cross-sectional inferences that do not take into account the fact that reported vitamin C intake on a food survey delivered retrospectively may not be the same as actual time-based plasma levels are indicated. Since its effects may be both disease specific, as well as dose-dependent and take weeks or months to unfold and be influenced by gender among other factors such as age and health and disease status, more data as to the importance of these interactive factors are strongly advocated [54]. It also appears that the efficacy of tailoring doses for reducing osteoarthritis pain and moderating its development as well as its adjunctive role in mediating pain holds promise and should be carefully examined.
Conclusion
In accord with past research efforts, it seems reasonable to conclude that osteoarthritis pathology and its pain, whether at the knee joint or any other joints, such as the shoulder, may be influenced in multiple respects by the presence or absence of optimal vitamin C levels, even if not favorably viewed in this regard in all instances and where results may depend largely on the study design [60]. Until more is known, however, it seems possible to avert the degree of projected future suffering and costs associated with shoulder osteoarthritis and its severity among older adults with this condition (Table 1).
As per Burton and McCormack [40] their pain-relieving, anti-inflammatory, and structural tendon effects may augment the positive functional outcomes gained from progressive exercise rehabilitation. it is also clear that the role and possible impact of varying vitamin C levels not only influences osteoarthritis risk, as well as osteoarthritic pain and its pathology, but at the shoulder, chances of a secondary disabling frozen shoulder state post-surgery or trauma [59]. However, there is clearly a need to examine and analyze this in a more substantive and robust manner, including the differential impacts of various dosages and forms of delivering vitamin C in various shoulder osteoarthritis subgroups of differing degrees. These may include independent or comparable efficacy studies to examine the unique benefits and risks of –
• Vitamin C and injury risk and recovery
• Shoulder surgery need and outcomes versus vitamin C
• Oral vitamin C supplements and combinations of these versus intra-articular injections or delivery or laser facilitated trans dermal delivery repair [42]
• Vitamin C rotator cuff tendon repair, and enhanced gene/ cell signaling potential [69]
• Vitamin C dosages and pain links
• Exercise associated muscle recovery and adaptation and vitamin C [70]
While requiring considerable time, funding, and dedication, chemically identified as ascorbic acid, data confirming vitamin C deficits have the potential to play a salient role in raising the risk for intractable destruction issues and possibly for repairing these is desirable if its presence can mitigate some degree of suffering [67,68]. In the interim it appears reasonable to suggest steps should be taken where indicated to assure older adults have access to sources of vitamin C and are able to maintain optimal vitamin C levels especially in the face of severe stress, neuropathic type pain – and rotator cuff tendon tears that can combine their destructive forces [23].
Benefits other than pain may include cartilage repair, bone maintenance, wound healing, collagen production, neural regeneration, muscle atrophy prevention, enhanced free radical scavenging, and antioxidant processes. Alone or in combination vitamin C presence may 1) enhance overall wellbeing and reduce suffering, 2) offer a low cost widely available safe option for physically, and economically vulnerable older adults suffering from shoulder trauma or osteoarthritis or both 3) reduce cases of older adult sufferers requiring placements, narcotics, or daily services, 4) foster more rapid and overall surgical recovery rates and fewer complications and infections 5) engender fewer overall demands on health providers amidst shrinking resources and budgets.
References
- Coppola C, et al. Osteoarthritis: insights into diagnosis, pathophysiology, therapeutic avenues, and the potential of natural extracts. Curr Issues Mol Biol. 2024; 46: 4063-4105.
- Meier MP, et al. Retrospective MRI analysis of 418 adult shoulder joints to assess the physiological morphology of the glenoid in a low-grade osteoarthritic population. BMC Med Imaging. 2025; 25: 35.
- Dunlap B, et al. Vitamin C supplementation for the treatment of osteoarthritis: perspectives on the past, present, and future. Ther Adv Chronic Dis. 2021; 12: 20406223211047026.
- Yamamoto N, et al. Non-operative management of shoulder osteoarthritis: current concepts. Jt Dis Orthop Sports Med. 2023; 8: 289-295.
- Tang P, et al. Ascorbic acid attenuates multifidus muscles injury and atrophy after posterior lumbar spine surgery by suppressing inflammation and oxidative stress in a rat model. Spine. 2018; 43: E1249-E1259.
- Crisol M, et al. Antioxidant additives reduce reactive oxygen species production in articular cartilage during exposure to cryoprotective agents. Cryobiology. 2020; 96: 114-121.
- Martel M, et al. Does vitamin C supplementation improve rotator cuff healing? A preliminary study. Eur J Orthop Surg Traumatol. 2022; 32: 63-70.
- Ballaz SJ, Rebec GV. Neurobiology of vitamin C: expanding the focus from antioxidant to endogenous neuromodulator. Pharmacol Res. 2019; 146: 104321.
- Maxfield L, et al. Vitamin C deficiency. StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Nov 12.
- Kim JR, et al. Therapeutics in osteoarthritis based on an understanding of its molecular pathogenesis. Int J Mol Sci. 2018; 19: E674.
- Stanborough RO, et al. Shoulder osteoarthritis. Radiol Clin North Am. 2022; 60: 593-603.
- DePhillipo NN, et al. Efficacy of vitamin C supplementation on collagen synthesis and oxidative stress after musculoskeletal injuries: a systematic review. Orthop J Sports Med. 2018; 6: 2325967118804544.
- Lewis LN, et al. Lower dietary and circulating vitamin C in middleand older-aged men and women are associated with lower estimated skeletal muscle mass. J Nutr. 2020; 150: 2789-2798.
- Marks R. Vitamin C and osteoarthritis: mini review and commentary. CPQ Orthop. 2018; 1: 1-16.
- Marks R. Global burden of osteoarthritis and vitamin C research trends, disease consequences, and implications. Int J Clin Med Case Rep. 2024; 42: 2.
- Frediani JK, et al. The role of diet and non-pharmacologic supplements in the treatment of chronic neuropathic pain: a systematic review. Pain Pract. 2024; 24: 186-210.
- Ali A, et al. A bioactive and biodegradable vitamin C stearatebased injectable hydrogel alleviates experimental inflammatory arthritis. Biomater Sci. 2024; 10: 39/d4bm00243a.
- Xu C, et al. Role of dietary patterns and factors in determining the risk of knee osteoarthritis: a meta-analysis. Mod Rheumatol. 2022; 32: 815-821.
- Schwartz ER, Adamy L. Effect of ascorbic acid on arylsulfatase activities and sulfated proteoglycan metabolism in chondrocyte cultures. J Clin Invest. 1977; 60: 96-106.
- Mattiuzzo E, et al. In vitro effects of low doses of β-caryophyllene, ascorbic acid and d-glucosamine on human chondrocyte viability and inflammation. Pharmaceuticals (Basel). 2021; 14: 286.
- Shivnath N, et al. Solanum xanthocarpum fruit extract promotes chondrocyte proliferation in vitro and protects cartilage damage in collagenase induced osteoarthritic rats. J Ethnopharmacol. 2021; 274: 114028.
- Abpeikar Z, et al. Characterization of macroporous polycaprolactone/silk fibroin/gelatin/ascorbic acid composite scaffolds and in vivo results in a rabbit model for meniscus cartilage repair. Cartilage. 2021; 13: 1583S-1601S.
- Vaysman M, et al. Pharmacologic enhancement of rotator cuff repair: a narrative review. Orthop Rev (Pavia). 2022; 14: 37782.
- Takisawa S, et al. Vitamin C is essential for the maintenance of skeletal muscle functions. Biology (Basel). 2022; 11: 955.
- Takisawa S, et al. Vitamin C deficiency causes muscle atrophy and a deterioration in physical performance. Sci Rep. 2019; 9: 4702.
- Luo TD, et al. Ascorbic acid and its clinical role in orthopaedic surgery. J Surg Orthop Adv. 2018; 27: 261-268.
- Laumonerie P, et al. Influence of vitamin C on the incidence of CRPS-I after subacromial shoulder surgery. Eur J Orthop Surg Traumatol. 2020; 30: 221-226.
- Hosseini-Monfared P, et al. Ascorbic acid reduces the blood loss after total knee arthroplasty: insights from a randomized controlled trial. Arthroplasty Today. 2025; 32: 101618.
- Oakes B, et al. Vitamin C in orthopedic practices: current concepts, novel ideas, and future perspectives. J Orthop Res. 2021; 39: 698-706.
- Noriega-González DC, et al. Effect of vitamin C on tendinopathy recovery: a scoping review. Nutrients. 2022; 14: 2663.
- Chiu PR, et al. Vitamin C protects chondrocytes against monosodium iodoacetate-induced osteoarthritis by multiple pathways. Int J Mol Sci. 2016; 18: E38.
- Zhou M, et al. ROS-induced imbalance of the miR-34a-5p/SIRT1/ p53 axis triggers chronic chondrocyte injury and inflammation. Heliyon. 2024; 10: e31654.
- Uehara H, et al. The effect of vitamin C and N-Acetylcysteine on tendon-to-bone healing in a rodent model of rotator cuff repair. Am J Sports Med. 2023; 51: 1596-1607.
- Bryer SC, Goldfarb AH. Effect of high dose vitamin C supplementation on muscle soreness, damage, function, and oxidative stress to eccentric exercise. Int J Sport Nutr Exerc Metab. 2006; 16: 270-280.
- Aïm F, et al. Efficacy of vitamin C in preventing complex regional pain syndrome after wrist fracture: a systematic review and meta-analysis. Orthop Traumatol Surg Res. 2017; 103: 465-470.
- Riffel APK, et al. Treatment with ascorbic acid and α-tocopherol modulates oxidative-stress markers in the spinal cord of rats with neuropathic pain. Braz J Med Biol Res. 2018; 51: e7097.
- Morikawa D, et al. Antioxidant treatment with vitamin C attenuated rotator cuff degeneration caused by oxidative stress in Sod1-deficient mice. JSES Open Access. 2018; 2: 91-96.
- Zără-Dănceanu CM, et al. Magnetic nanoemulsions for the intraarticular delivery of ascorbic acid and dexamethasone. Int J Mol Sci. 2023; 24: 11916.
- Burger MG, et al. Ascorbic acid attenuates senescence of human osteoarthritic osteoblasts. Int J Mol Sci. 2017; 18: 2517.
- Burton I, McCormack A. Nutritional supplements in the clinical management of tendinopathy: a scoping review. J Sport Rehabil. 2023; 32: 493-504.
- D’Aniello C, et al. Vitamin C in stem cell biology: impact on extracellular matrix homeostasis and epigenetics. Stem Cells Int. 2017; 2017: 8936156.
- Huang T-L, et al. Synergistic effect of l-ascorbic acid and hyaluronic acid on the expressions of matrix metalloproteinase-3 and -9 in human chondrocytes. J Biomed Mater Res B Appl Biomater. 2018; 106: 1809-1817.
- Liao Z, et al. Intra-articular injection of ascorbic acid/ferric chloride relieves cartilage degradation in rats with osteoarthritis. J South Med Univ. 2018; 38: 62-68.
- Qamar R, et al. Exploring ascorbic acid’s role in orthopedic practices: present theories, innovative approaches, and prospects. Cureus. 2024; 16: e60164.
- Surapaneni KM, Venkataramana G. Status of lipid peroxidation, glutathione, ascorbic acid, vitamin E and antioxidant enzymes in patients with osteoarthritis. Indian J Med Sci. 2007; 61: 9-14.
- Zhang X, et al. Vitamin C regulates skeletal muscle post-injury regeneration by promoting myoblast proliferation through its direct interaction with the Pax7 protein. Food Funct. 2024; 15: 4575-4585.
- Röhr D, et al. Sodium-dependent vitamin C transporter 2 deficiency impairs myelination and remyelination after injury: roles of collagen and demethylation. Glia. 2017; 65: 1186-1200.
- Lindsey RC, et al. Vitamin C effects on 5-hydroxymethylcytosine and gene expression in osteoblasts and chondrocytes: potential involvement of PHD2. PLoS One. 2019; 14: e0220653.
- Mallah A, et al. Sex-specific reduction in inflammation of osteoarthritic human chondrocytes and nutraceutical-dependent extracellular matrix formation. J Immunol Regen Med. 2021; 14: 100054.
- Park CY, Shin S. Low dietary vitamin C intake is associated with low muscle strength among elderly Korean women. Nutr Res (New York). 2024; 127: 75-83.
- Filho AVN, et al. Vitamin C protects against doxorubicin-induced skeletal muscle atrophy: role of oxidative stress. Can J Physiol Pharmacol. 2025; 103: 200-207.
- Leboy PS, et al. Ascorbic acid induces alkaline phosphatase, type X collagen, and calcium deposition in cultured chick chondrocytes. J Biol Chem. 1989; 264: 17281-17286.
- Röhr D, et al. Sodium-dependent vitamin C transporter 2 deficiency impairs myelination and remyelination after injury: roles of collagen and demethylation. Glia. 2017; 65: 1186-1200.
- Lindsey RC, et al. Vitamin C effects on 5-hydroxymethylcytosine and gene expression in osteoblasts and chondrocytes: potential involvement of PHD2. PLoS One. 2019; 14: e0220653.
- Mobasheri A, et al. Glucose transport and metabolism in chondrocytes: a key to understanding chondrogenesis, skeletal development and cartilage degradation in osteoarthritis. Histol Histopathol. 2002; 17: 1239-1267.
- Joseph GB, et al. Associations between vitamins C and D intake and cartilage composition and knee joint morphology over 4 years: data from the Osteoarthritis Initiative. Arthritis Care Res (Hoboken). 2020; 72: 1239-1247.
- Tang P, et al. Ascorbic acid attenuates multifidus muscles injury and atrophy after posterior lumbar spine surgery by suppressing inflammation and oxidative stress in a rat model. Spine. 2018; 43: E1249-E1259.
- Laumonerie P, et al. Influence of vitamin C on the incidence of CRPS-I after subacromial shoulder surgery. Eur J Orthop Surg Traumatol. 2020; 30: 221-226.
- Feusi O, et al. Vitamin C as a potential prophylactic measure against frozen shoulder in an in vivo shoulder contracture animal model. Am J Sports Med. 2023; 51: 2041-2049.
- Tarara DT, Smoliga JM. Does vitamin C improve rotator cuff healing? It depends on how one interprets p values. Eur J Orthop Surg Traumatol. 2022; 32: 583-584.
- Liu X, et al. Mechanism and potential of vitamin C supplementation in sarcopenia prevention and treatment. Chin J Tissue Eng Res. 2024; 28: 4405.
- Zhang H, et al. Vitamin C intake and osteoarthritis: findings of NHANES 2003–2018 and Mendelian randomization study. Front Nutr. 2024; 11: 1409578.
- Peregoy J, Wilder FV. The effects of vitamin C supplementation on incident and progressive knee osteoarthritis: a longitudinal study. Public Health Nutr. 2011; 14: 709-715.
- Dincel YM, et al. Effects of high-dose vitamin C and hyaluronic acid on tendon healing. Acta Ortop Bras. 2018; 26: 82-85.
- Oh J, Lee MK. Shoulder pain, shoulder disability, and depression as serial mediators between stress and health-related quality of life among middle-aged women. Health Qual Life Outcomes. 2022; 20: 142.
- Mohammadivahedi F, et al. Comparative efficacy of plateletrich plasma (PRP) injection versus PRP combined with vitamin C injection for partial-thickness rotator cuff tears: a randomized controlled trial. J Orthop Surg Res. 2024; 19: 426.
- Chang Z, et al. Ascorbic acid provides protection for human chondrocytes against oxidative stress. Mol Med Rep. 2015; 12: 7086-7092.
- Hart A, et al. The role of vitamin C in orthopedic trauma and bone health. Am J Orthop (Belle Mead NJ). 2015; 44: 306-311.
- Das S, et al. Nickel and oxidative stress: cell signaling mechanisms and protective role of vitamin C. Endocr Metab Immune Disord Drug Targets. 2020; 20: 1024-1031.
- Kim J. Effect of high-dose vitamin C and E supplementation on muscle recovery and training adaptation: a mini review. Phys Act Nutr. 2023; 27: 8.