Volume 1, Issue 2
Article Type: Short Commentary
The antithrombotic prescription in the elderly dizzy patient: Newest paradigms
Neto ACL, PhD*; Bittar RSM, PhD
Department of Otorhinolaryngology, University of São Paulo, São Paulo, Brazil.
*Corresponding author: Neto ACL
Department of Otorhinolaryngology, University of São Paulo,
Av. Doutor Enéas Carvalho de Aguiar, 255, Cerqueira Cesar, São Paulo 05403900, Brazil
Email ID: aclimanetoent@gmail.com
Tel: +55-11-3088-0299
Received: Sep 15, 2025
Accepted: Oct 06, 2025
Published Online: Oct 13, 2025
Journal: Annals of Gerontology and Geriatrics
Copyright: Neto ACL et al. © All rights are reserved
Citation: Neto ACL, Bittar RSM. The antithrombotic prescription in the elderly dizzy patient: Newest paradigms. Ann Gerontol Geriatr Res. 2025; 1(2): 1022.
Introduction
Episodic vertigo and dizziness of vascular origin are common presentations in the Emergency Department (ED) and outpatient settings. In 2022, the Bárány Society proposed formal definitions and diagnostic criteria for Vascular Vertigo and Dizziness (VVD), which encompasses strokes and Transient Ischemic Attacks (TIAs) involving the Vertebrobasilar (VB) circulation; isolated labyrinthine infarction or hemorrhage; and vertebral artery compression syndrome [1].
Despite recommendations for a parsimonious prescribing of antiplatelets and anticoagulants for elderly patients [2], recent neurotology publications have highlighted the clinical features and best practices for managing VVD in the elderly. This brief communication emphasizes the importance of timely recognition and initiation of secondary prophylactic treatment. It aims to alert readers to these new concepts, in which dizziness and vertigo are red flags of ischemic events.
VVD clinic features
VVD should be considered in patients presenting with episodic vertigo, dizziness, or unsteadiness, particularly when accompanied by any of the following:
- Focal central neurological symptoms (e.g., hemiparesis, sensory loss, dysarthria, dysphagia) or severe truncal ataxia/ postural instability during the episode;
- New-onset moderate to severe craniocervical pain occurring
- Simultaneously with the attack;
- High vascular risk, such as an ABCD² score ≥ 4 or a diagnosis of atrial fibrillation;
- Neuroimaging evidence of acute ischemia on cranial MRI, especially on Diffusion-Weighted Imaging (DWI-MRI);
- Vascular imaging findings showing significant (>50%) stenosis of a vertebrobasilar artery;
- Or isolated spontaneous episodic vertigo in older adults for whom no other plausible cause can be identified [1].
In a prospective cohort of 103 patients with VBTIA followed over a median period of 12 months, imbalance (46.7%) and vertigo (39.8%) were the most frequently reported symptoms. The duration of attacks was less than 1 minute in 33.9% of cases, 1-10 minutes in 33.0%, 10-60 minutes in 14.6%, and more than 60 minutes in 18.5%. Triggering factors were referred by 19.4%, including eccentric neck positioning, physical exertion, and postural changes. The most frequently associated symptoms were transient visual loss (30%), syncope (27.2%), diplopia (10.7%), balance-related falls/drop attacks (9.7%), dysphagia (5.8%), and new-onset cranial pain (4.8%), although 15.5% of patients reported no accompanying symptoms. A noteworthy finding was the recurrence of events, with approximately 69% of patients experiencing more than one attack per month. The infratentorial region’s high white matter proportion and vascular distribution may be responsible for this phenomenon, and may favor this area for TIA rather than stroke [3]. This anatomical background probably explains why isolated transient neurological attacks in the VB territory, such as vertigo and dizziness, are about 15 times more likely to precede a VB stroke than a carotid stroke [4].
Among the various algorithms for diagnosing dizziness in the ED setting, the common bases are recognizing central findings in HINTS (Head Impulse test, evaluation of Nystagmus, and Skew Deviation), as well as detecting positional nystagmus and truncal ataxia. With the presence of findings that cannot be explained by an inner ear disease, the diagnosis of VVD must be considered. However, the accurate application and interpretation of these bedside tests require specific training and clinical experience on the part of emergency physicians [5-7].
Antithrombotic treatment
Based on the above-mentioned clinical features, if a VVD attack is suspected and it is understood that the dizziness, vertigo, or unsteadiness are due to a probable cerebrovascular event, therapeutic management should begin immediately.
In the ED setting, if a patient is diagnosed with vertigo or dizziness due to a stroke, the possibility of thrombolysis or thrombectomy must always be evaluated, if available. It’s important to note that the acceptable time window for a VB stroke is longer than for a carotid stroke [8].
If there are no indications for reperfusion therapy, it is recommended that antiplatelet therapy be started while other tests and evaluations are being performed [3]. (Figure 1) illustrates how our group has managed these patients.
When indicated, Double Antiplatelet Therapy (DAPT) should be prescribed for up to 90 days following an attack [9]. However, there is still limited literature regarding patients who relapsed when they returned to monotherapy and patients who were already using antithrombotics before the crisis.
In the prospective cohort mentioned above (mean age 70.9±9.3 years), treatment regimens included aspirin (55.3%), clopidogrel (18.5%), aspirin plus clopidogrel (24.3%), and rivaroxaban (1.9%). Among these, 18.5% were already on monotherapy and had their regimen escalated to DAPT. During a median follow-up of 12 months (range: 2-36), the frequency of attacks was reduced by 93.2% [95% CI: 88.34-98.06; number needed to treat=1]. Only seven patients (6.8%) experienced a recurrent attack while on medication. No major side effects were observed [3].
Conclusion
VVD is an important cause of episodic vertigo and dizziness, particularly in older adults. Prompt recognition based on clinical features and bedside testing, followed by early initiation of antiplatelet therapy can significantly reduce recurrence of events and prevent stroke. Although parsimonious prescribing of antiplatelets and anticoagulants is recommended for elderly patients, antithrombotic therapy is fundamental for VVD.
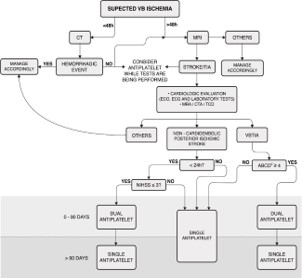
This algorithm was not applicable to patients receiving acute thrombolysis. Laboratory tests included complete blood count, troponin, prothrombin time, partial thromboplastin time, glucose, hemoglobin A 1c, creatinine, and fasting and non-fasting lipid profiles.
MRI: Cranial Diffusion-Weighted Magnetic Resonance; VB: Vertebrobasilar; CT: Cranial Computed Tomography; ECO: Echocardiography; ECG: Electrocardiogram; MRA: Cranial and Cervical Magnetic Resonance Angiography; CTA: Cranial and Cervical Computed Tomography; TCD: Transcranial Doppler Ultrasonography; VBTIA: Vertebrobasilar Transient Ischemic Attack; NIHSS: National Institutes of Health Stroke Scale.
References
- Kim JS, Newman-Toker DE, Kerber KA, Jahn K, Bertholon P, Waterston J, et al. Vascular vertigo and dizziness: diagnostic criteria: consensus document of the committee for the classification of vestibular disorders of the Bárány society. J Vestib Res. 2022; 32: 205-222.
- Davidson KW, Barry MJ, Mangione CM, Cabana M, Chelmow D, Coker TR, et al. US Preventive Services Task Force. Aspirin use to prevent cardiovascular disease: US Preventive Services Task Force recommendation statement. Jama. 2022; 327: 1577-1584.
- Neto ACL, Kim JS, Bernardo WM, Bittar RSM. Vertigo and dizziness due to vertebrobasilar TIA: a prospective study. Front Stroke. 2024; 3: 1429068.
- Paul NLM, Simoni M, Rothwell PM. Transient isolated brainstem symptoms preceding posterior circulation stroke: a populationbased study. Lancet Neurol. 2013; 12: 65-71.
- Edlow JA, Carpenter C, Akhter M, Khoujah D, Marcolini E, Meurer WJ, et al. Guidelines for reasonable and appropriate care in the emergency department 3 (GRACE-3): acute dizziness and vertigo in the emergency department. Acad Emerg Med. 2023; 30: 442-486.
- Filippopulos FM, Strobl R, Belanovic B, Dunker K, Grill E, Brandt T, et al. Validation of a comprehensive diagnostic algorithm for patients with acute vertigo and dizziness. Eur J Neurol. 2022; 29: 3092-3101.
- Koohi N, Male AJ, Kaski D. Acute positional vertigo in the emergency department—peripheral vs central positional nystagmus. Front Neurol. 2023; 14: 1266778.
- Knapen RR, Frol S, van Kuijk SM, Oblak JP, van der Leij C, van Oostenbrugge RJ, et al. Intravenous thrombolysis for ischemic stroke in the posterior circulation: a systematic review and meta-analysis. J Stroke Cerebrovasc Dis. 2024; 33: 107641.
- Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke. 2021; 52: e364-e467.